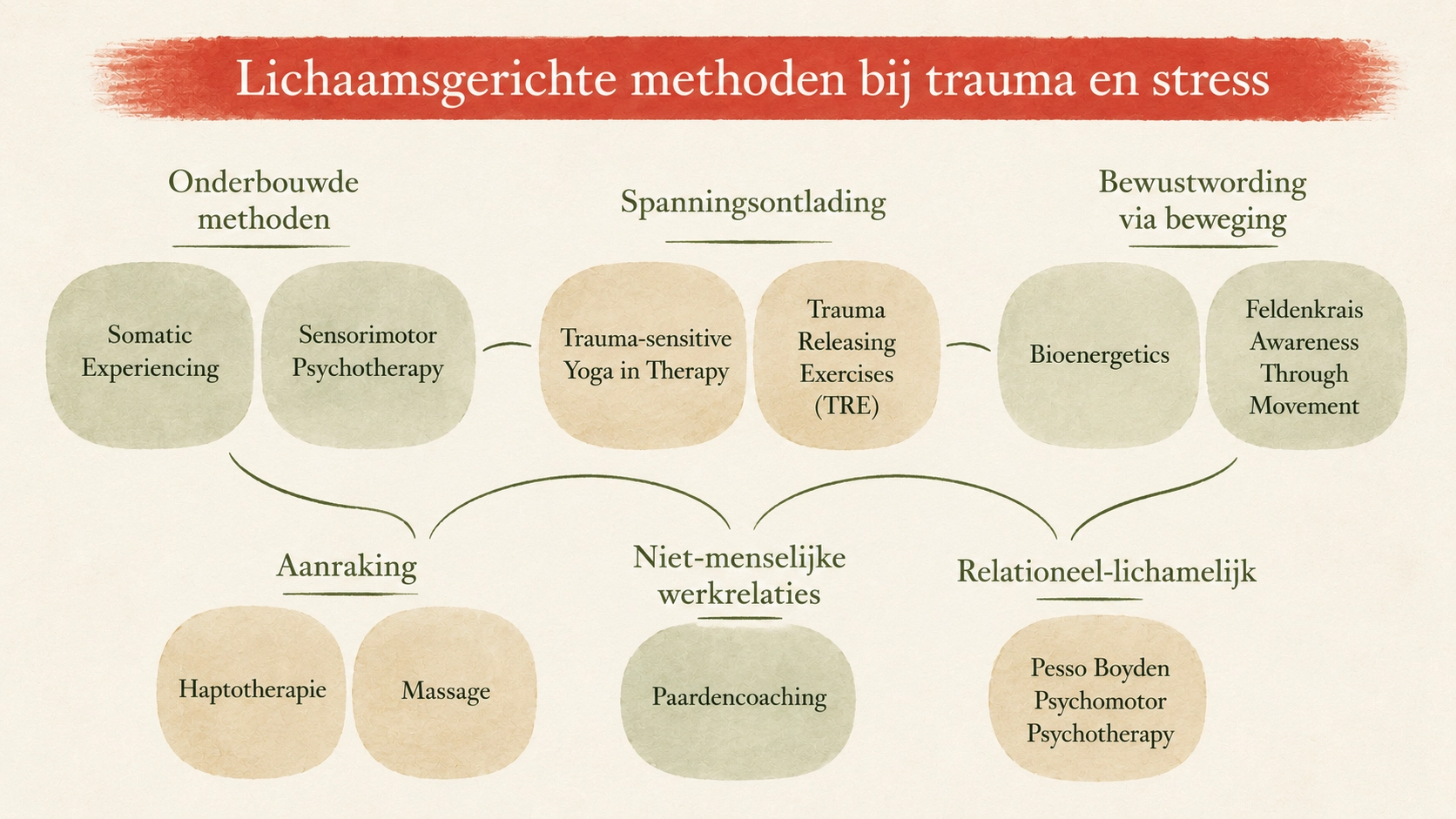
Anyone working with PTSD or moral injury will eventually hear that the body is part of the picture. Trauma becomes embedded in the nervous system, in muscle tension, breathing, and posture. Not as a metaphor, but as a physiological reality. What is harder to find is an honest overview of what “body-oriented therapy” actually means in practice. The term covers a broad spectrum of approaches — from clinically well-supported methods to more experimental work, from psychotherapy with body awareness to working with horses.
This post tries to provide that overview. Not as a ranking and not as a complete map, but as a guide. One paragraph per approach: what it is, what it does in the body, who it may fit, and where nuance matters.
One more thing worth mentioning. Some of the methods below I have personally experienced; others I know through literature and clinical research. Where I have personal experience, I mention it explicitly. And for all approaches discussed here: they exist alongside specialized trauma treatment, not as a replacement for it.
Evidence-based trauma-specific methods#
Somatic Experiencing (Peter Levine)#
Peter Levine developed Somatic Experiencing from the observation that wild animals rarely develop chronic trauma, despite living under constant threat of death. Humans often do. In many cases because they suppress the body’s natural discharge response after danger. Somatic Experiencing works through “titration”: small, manageable doses of activated bodily sensation alternating with moments of safety. Gradually, the nervous system relearns how to move between activation and recovery.
A substantial amount of research has now been done on the method. It shows positive effects for PTSD. For people who have already gone through extensive talk therapy without sufficient results, this can be a valuable addition.
Sensorimotor Psychotherapy (Pat Ogden)#
Pat Ogden combines psychotherapy with systematic body awareness. Thoughts, emotions, and bodily sensations are not treated separately but tracked simultaneously. The client learns to notice what the body is doing while speaking — shoulders tightening, breath stopping, a knee pulling away — and what those signals reveal beneath the words.
The method is well grounded and internationally used within accredited trauma treatment programs. For clients who are willing to talk but sense that words alone are not enough, this is often a natural next step.
Trauma-Sensitive Yoga (David Emerson and Bessel van der Kolk)#
Trauma-sensitive yoga is not an ordinary yoga class. There is no physical adjustment, no mandatory posture, and the instructor is trained not to use language that implies control or correction. The client is invited to choose for themselves in every posture. That may sound minor, but it is fundamental: for people whose trauma involved losing choice and bodily autonomy, this form restores precisely that.
The work of David Emerson and Bessel van der Kolk (Trauma Center, Boston) has made this one of the best-supported body-based interventions for people with complex PTSD.
Releasing tension through the body#
TRE — Tension and Trauma Releasing Exercises (David Berceli)#
David Berceli developed TRE in war zones, where large groups of people were traumatized simultaneously and had no access to individual therapy. The method consists of a series of exercises designed to trigger the body’s natural tremoring response. A neurogenic mechanism also seen in animals that helps discharge accumulated stress energy.
My own experience: I followed TRE sessions at Yogalab in Amsterdam. It brought noticeable relaxation into the body. The peer-reviewed research is still limited, and the method is sometimes promoted too casually, but for those it works for, the effect is direct and physically tangible.
Bioenergetics (Alexander Lowen)#
Alexander Lowen expanded on Wilhelm Reich’s idea that unresolved emotions become stored in the body as “armor” — chronic muscular tension. Bioenergetic exercises use specific postures, breathing exercises, and sometimes expressive movement to release that trapped energy.
I do not personally have practical experience with this method. Conceptually, it aligns with TRE and Somatic Experiencing. All three work with bodily discharge of what the nervous system could not process independently. The peer-reviewed research is more limited than for the previously mentioned methods, yet Bioenergetics has a long clinical tradition and directly addresses physically held tension.
Awareness through movement#
Feldenkrais (Moshe Feldenkrais)#
Moshe Feldenkrais developed a method using extremely subtle movements to reorganize motor patterns and self-perception. The focus is not symptom reduction but learning: the body discovers new possibilities of movement, and with that, the way you inhabit your body changes as well.
I personally practiced Feldenkrais for a period during treatment. For me, it did less than TRE. That probably says more about my specific nervous system than about the method itself. There are people for whom Feldenkrais fits exactly what they need. Research mainly exists around chronic pain and posture, less directly around PTSD.
Touch and body tissue#
Haptotherapy (Frans Veldman)#
I received haptotherapy for a year. It made me touchable again.
That is the shortest summary of what haptotherapy can do in PTSD. For people for whom touch no longer feels natural, or no longer felt possible at all. Frans Veldman developed haptonomy in the Netherlands; haptotherapy is its therapeutic application. The method works through touch within an explicitly relational context: through physical contact, the therapist reads what the body communicates and carefully builds trust. For people who have physically “shut down” because of moral injury, attachment trauma, or relational trauma, this can offer an opening that talk therapy alone often cannot provide.
Clinical experience with haptotherapy in PTSD is extensive; peer-reviewed research remains more limited than with Somatic Experiencing or trauma-sensitive yoga. The Dutch Association of Haptotherapists has a useful background publication on haptotherapy for PTSD (PDF).
Connective tissue massage and trauma-informed bodywork#
Massage is not a complete therapy for PTSD, but it is an underestimated form of support. As a certified sports massage therapist myself, I know what good connective tissue massage can release. Tension that has structurally immobilized part of the body for years can become accessible again under skilled hands.
An important nuance: without trauma awareness on the part of the massage therapist, release can also become destabilizing. If a memory suddenly surfaces or a client becomes emotionally overwhelmed, the therapist needs to know what they are doing. A trauma-informed massage therapist is not the same as an experienced technician. If you are considering this route: explicitly ask about experience with PTSD clients and build up slowly.
Non-human working relationships#
Equine-Assisted Therapy / Horse Coaching#
Horses read bodily tension better than most people. They respond directly to what is happening in your nervous system, even when you yourself do not yet realize it. Because of that, the horse becomes a mirror not metaphorically, but concretely observable.
I participated twice in horse coaching sessions through the BNMO. It brought a great deal of relaxation. For people who have lost language around their experience, or for whom therapy feels too confrontational, working with a horse can provide access that does not depend on words. Research into equine-assisted therapy for veterans and people with complex PTSD is growing.
Relational and bodily#
Pesso Boyden System Psychomotor (PBSP)#
Albert Pesso and Diane Boyden developed a method that works bodily around unmet developmental needs: place, protection, care, boundaries, recognition. In group structures, what was missing in someone’s history is represented symbolically and physically.
It is a niche method, but conceptually very close to what plays out in moral injury and attachment trauma: not only what happened, but what should have happened and never came. For clients who feel their pain is not just about an event but about an absence, this can be an exceptionally fitting approach.
Safety around touch#
In every method where touch plays a role: haptotherapy, massage, some forms of Somatic Experiencing, sometimes equine-assisted work. Safety is not a detail but the basic condition. For people with a history of sexual trauma or physical violence, the wrong kind of touch can become activating again instead of regulating.
There are three things I personally consider important here.
First: trauma-specific training of the practitioner. A skilled haptotherapist without trauma knowledge is different from one who has worked with PTSD clients for years. Ask explicitly about experience with this population. A serious practitioner answers that question without hesitation.
Second: consent and stop signals. A trauma-informed therapist works with explicit consent around touch and respects “stop” as a word requiring no further explanation. Anyone who does not is simply not the right practitioner, regardless of technical skill.
Third: the difference between being touched by someone who can read your nervous system versus someone who only masters their method. In body-oriented therapy even more than in talk therapy, the therapeutic fit is not a luxury, it is a functional part of what makes the method work.
How do you choose?#
Four questions you can ask yourself before starting. Do you feel a genuine connection with the practitioner? Not just liking them, but feeling safe enough to show something vulnerable? Does the intensity of the method fit where you currently are? Do not start with the heaviest approach if you have only just come out of crisis. Does touch work for you, or is a non-touch method (trauma-sensitive yoga, Feldenkrais, equine-assisted therapy) a better entry point? And finally: does the therapist specifically have trauma experience, or are they mainly a specialist in their method without trauma focus?
None of these questions has a right or wrong answer. They are simply questions that help orient you.
What this overview does not do#
No ranking. The order of the modalities is logical. Beginning with the best-supported approaches and moving toward more specific or niche methods. But that does not mean the first is automatically best for you.
No complete inventory. Craniosacral therapy, Rolfing, holotropic breathwork, and several other approaches are intentionally not included. Not because they are necessarily poor methods, but because I do not have enough experience or confidence in them to say something useful here.
No replacement for specialized trauma care. For severe PTSD and moral injury, well-trained trauma therapists often in combination with EMDR or CBT remain the foundation. Body-oriented approaches exist alongside that, sometimes within it, rarely instead of it.
Related reading#
- Trauma and the body
- Porges’ Polyvagal Theory
- Breathing and PTSD
- Exercise and PTSD
- The Rule of Four and trauma
- Shame after trauma
Conclusion: the body as an entry point#
What all these methods share, despite their differences, is a simple premise: the body is not a passive vehicle carrying the consequences of trauma, but an active conversation partner in recovery. The techniques differ. The scientific support differs. The style differs. But the foundation remains the same. What the body holds, the body can also help release.
Which method fits you is not simply a matter of what performs best in research, but what connects with your nervous system, your history, and the people you work with. Sometimes that is one method that accompanies you for years. Sometimes it is a combination. Sometimes it is precisely the method you never expected would work for you, yet turns out to provide exactly the access you needed.
The body waits. Starting there is usually the hardest step.
Sources and scientific publications#
- Levine, P. (1997). Waking the Tiger — Healing Trauma
- Levine, P. (2010). In an Unspoken Voice — How the Body Releases Trauma and Restores Goodness
- Ogden, P., Minton, K. & Pain, C. (2006). Trauma and the Body — A Sensorimotor Approach to Psychotherapy
- Van der Kolk, B. (2014). The Body Keeps the Score
- Emerson, D. (2015). Trauma-Sensitive Yoga in Therapy
- Berceli, D. (2005). Trauma Releasing Exercises (TRE)
- Lowen, A. (1975). Bioenergetics
- Feldenkrais, M. (1972). Awareness Through Movement
- Veldman, F. (1988). Haptonomy — Science of Affectivity
- Dutch Association of Haptotherapists — Haptotherapy and PTSD (PDF)
Questions?#
Do you recognize this in yourself or in your work with others? Use the contact form to get in touch with me.